



 Talk about trying to hide bad news on a Friday night.
Talk about trying to hide bad news on a Friday night.
Sanofi-Aventis sent out two press releases on Friday afternoon, one announcing that it was submitting updated safety data on its blighted rimonabant (approved last year in Europe as Acomplia) to the European authorities, and the other to say that it’s withdrawing its US NDA for the drug.
Neither is particularly surprising. Of course EMEA is “reviewing the available data on psychiatric events” associated with the drug. There are 200,000 patients in Europe taking a compound that 14 US experts unanimously judged unfit for approval in an advisory committee vote earlier in June. (An outcome which, as my colleague argues this month in The RPM Report, wasn’t particularly surprising either.)
Judging from the Q&A session on the conference call—held at 6pm Paris time, about an hour after we received the press releases, but nevertheless caught by more analysts and journalists than Sanofi probably expected--there’s still some confusion over data. A meta-analysis of trial data studied by FDA advisors showed up some rather different results when it came to suicidality rates than those submitted in Sanofi-Aventis’ original package. “We disagree with the FDA analysis,” noted Marc Cluzel, SVP Science and Medical Affairs, on the call.
Still, the company has withdrawn its NDA filing, since, it feels, there wasn’t enough time to discuss with FDA the various points raised by the advisory committee before the July 26th PDUFA date.
Is it an admission of defeat? Not a bit, said the Sanofi SVPs. “We feel it’s our duty to try to allow US patients to benefit from such a drug. Unfortunately though there’s a misunderstanding” over its risk-benefit profile, the executives said.
Indeed there is. Sanofi still thinks it can get the drug approved for a subset of obese patients, those with various co-morbidities. It’s still downplaying the depression issue. Indeed, “we found that in animals models rimonabant even had anti-depressant activity,” noted Cluzel.
Nice try. But if rimonabant, a cannabinoid receptor antagonist, works by reversing the "munchies" effect associated with taking cannabis, it seems logical—quite apart from whoever’s data interpretation you believe--that it could also reverse the mood-enhancing effects, too. Either way, it’s clear that no one yet understands the cannabinoid system sufficiently well to be entirely sure. And that’s not a good situation to be in given today’s super-safety-conscious FDA. Indeed, as Cluzel acknowledged in the call, most of the key rimonabant trials "were done between 2001 and 2004, before Vioxx."
Though not impressed by Sanofi-Aventis’ Friday night trick, if that's what it was, IN VIVO Blog can only commend the company for keeping its chin up, publicly at least. Remember colorectal cancer drug oxaliplatin (Eloxatin), Cluzel pointed out: it got turned down in 1999 by an advisory committee, due to unconvincing data on survival benefit, but later, post re-submission, received one of the fastest approvals ever.
That was three years later, though. Rimonabant may yet arrive in the US, for some patient groups, but it won’t be in the second half of this year. Even data from the long-term Crescendo trial investigating the drug’s impact on cardiovascular events, due to report in 2010, may not do it--some advisory panel members said none of the ongoing trials of rimonabant are designed to provide sufficient clarity over adverse events. Much later than that (the drug’s key patent expires in Europe in 2019) and Sanofi-Aventis might just be moving straight onto its two back-up compounds.
Meantime, keep an eye out for a shopping bag marked ‘Bristol-Myers Squibb’.
Friday, June 29, 2007
Could've Seen That One Coming
Private Equity: Muscling in on Big Pharma at Biotech's High Rollers' Table
Talk about co-dependency. Pharma needs biotech’s products; biotech needs pharma’s cash. Oh, they say they need other things, but when it comes down to it – that’s about the equation. 
So if biotech had a different source of cash (or Pharma had a different source of products), well – this marriage would turn open.
That’s why private equity has become such an interesting game changer. PE firms, stuffed with too much cash as it is and incentivized with management fees to stuff themselves still further, are all chasing the same buyout opportunities, throwing ever greater sums at owners and managers in order to get into the deals.
Biotech, which certainly needs cash, doesn’t return money on anything like a PE firm’s preferred timeline. But biotechs are also relatively unmined territory. Therefore cheap. That’s why you’re beginning to see major private equity players doing things private equity rules say they shouldn’t do.
Consider this progression. In 2004, KKR put something like $200 million into Jazz Pharmaceuticals—a theoretically stable, spec pharma-ish kind of investment. The financing underwrote Jazz’s takeover of the commercial-stage Orphan Medical, so KKR at least got some cash flow, which PE investors like to see. And there was no discovery risk—but certainly development risk. (Not that it's worked out brilliantly, so far. See our recent post.)
Two years later, New Mountain enables the Ikaria/Ino deal – creating a theoretically self-financing company (like Jazz, it has a commercial organization providing the requisite cash flow) but it nonetheless depends for its success on the crapshoot of discovery.
And now The Invus Group is putting $205 million into Lexicon, with the potential to add another $345 million down the road. They’ll get a minimum of 40% of the company and could end up owning far more. But now the whole thing is based on discovery – and not just me-too discovery, but Lexicon’s novel-target, novel-compound approach (see our upcoming article in the July/August IN VIVO).
In short, private equity is moving into pharma territory, funding companies the way only pharmas once could. The whole point is to build organizations of such size that a biotech can do its deals on relatively equal terms with pharma – which means that if it doesn’t get its deal price, it can walk away and do its own development and commercialization, continuing to increase its assets’ value.
The theory underlying this game is that biotechs are still leaving way too much value on the negotiating table. That’s the value the PE investor needs to retain in order to counterbalance his basic disadvantage as a purely financial, not strategic, buyer. That strategic buyer—Big Pharma--can pay more for particular assets because they can do more with them (like shoring up a fading portfolio or keeping profitable and busy a sales they don’t want to lose). Can PE use its money to extract that strategic premium biotechs on their own can’t? It’s an interesting gamble: both biotech and Big Pharma need to get to know the new dice-throwers at the high-rollers’ table.
Thursday, June 28, 2007
Live from Paris: Roger's dealmaking overview
 Everyone was feeling a bit fuzzy this morning
Everyone was feeling a bit fuzzy this morning Drug Discovery Pays
Drug Discovery Pays Wednesday, June 27, 2007
In Our Face

The Natick, Mass. company reached an agreement to buy Remon Medical Technologies Inc., a privately held and venture-backed company based in Caesarea, Israel.
(We know. This is Karl Rove, not Jim Tobin.)
We may have more on the acquisition in the next START-UP. For now, here’s a quick Q&A with CEO Hezi Himelfarb and Terry McGuire, general partner at Polaris Venture Partners, one of Remon’s earlier investors. (Terms weren't disclosed, btw, but McGuire seemed very happy with the outcome.)
IN VIVO Blog: So who approached whom about merging?
McGuire: We already had relationship with Guidant that was going on a couple of years. And that turned out to be a prosperous relationship in the sense that we really developed some important technology that Boston Scientific recognized would continue to be important. And through the [Guidant] acquisition we got to know Boston Scientific even better and the time seemed right to talk about merging the companies.
IVB: Were there other opportunities for an exit? Did CardioMEMS failed IPO make a sale more appealing?
McGuire: CardioMEMS has a very different business model. CardioMEMS never entered into our relationship in any way. This acquisition was based on a relationship that had been evolving over two years. It’s what I would describe is a perfect baton pass. Here is this really innovative company and Boston Scientific saw what they could do with this. It was based on a long-term relationship. It really wasn’t based on the fact CardioMEMS did XYZ. Remon had a very strong balance sheet. It wasn’t like we needed to do anything.
IVB: Were there other options for Remon?
Himelfarb: We’ve been actually working on evaluating other [partnership] opportunities with other companies and there was a lot of interest in our technology because our technology is actually the only one today that provides real intrabody communication in a totally wireless manner …But eventually you can do such a deal with one company and luckily Boston Scientific was the one.
IVB: Where do you fit into BSX?
Himelfarb: Right now we are continuing exactly as we were. We continue to be in our facility which is located in Israel with the same employees, same management team. Everything actually remains the same. Then, probably again after a short-period of training and education we will find out what are the objectives. For now we are staying the same as before the acquisition.
IVB: Any changes within the next 12 months?
Himelfarb: I believe after they learn more about our technology they may do some changes in the focus of the company
Welcome to Paris: take my drug ... Please
 Mood lighting for the hot dealmaking topics panel
Mood lighting for the hot dealmaking topics panel
Still, oncology, the favorite specialist area for most companies, continues to dominate in number of deals. This is generally due to the availability of oncology products, thanks to the myriad targets and unmet need which make it a fertile ground for many biotech companies, points out Nigel Sheail.
Although biotech companies seemingly have the upper hand--at least as reflected by deal valuations--the panelists stressed that high-upfronts and big payoffs weren't necessarily the way forward for every deal, thanks to tax considerations etc. Partners should "be creative," think about downstream rights, quids, and revenue sharing. Scott Myers encouraged potential partners to dream up new structures: "don't expect us to have a formula, because we don't."
 All that said, IN VIVO Blog prefers for now to look at the numbers. If as Aesop (and today, Nigel Sheail) said, "the value is in the worth, not in the number," then surely as biotech's own products become more valuable to the future of Big Pharma that worth will increase. We think the numbers will continue to follow.
All that said, IN VIVO Blog prefers for now to look at the numbers. If as Aesop (and today, Nigel Sheail) said, "the value is in the worth, not in the number," then surely as biotech's own products become more valuable to the future of Big Pharma that worth will increase. We think the numbers will continue to follow.If you're here, happy dealmaking.
Tuesday, June 26, 2007
Roche to Ventana: We want you so bad
 It was apparent from today's Roche investor call that five months of trying to open acquisition discussions with Ventana Medical Systems has left the Swiss firm frustrated and desperate. It may well win the fair hand of Ventana with some combination of a carrot (we'd be so good together) and/or a stick (we're gonna get ya one way or the other), but by putting its cards on the table the way it has, Roche seems to have given Ventana all the leverage.
It was apparent from today's Roche investor call that five months of trying to open acquisition discussions with Ventana Medical Systems has left the Swiss firm frustrated and desperate. It may well win the fair hand of Ventana with some combination of a carrot (we'd be so good together) and/or a stick (we're gonna get ya one way or the other), but by putting its cards on the table the way it has, Roche seems to have given Ventana all the leverage.
Good Things Come
Six months have passed since the deal was first announced, but shareholders of Ithaka Acquisiton Corp., the special purpose acquisition company, last week agreed to the merger with Alsius Corp., the temperature control device company.
The merger gives the new entity--called Alsius Corp.--roughly $45 million in cash and a ticker on Nasdaq. We'll have a lot more on this IPO alternative and Alsius' future plans in our upcoming START-UP.
We'd love to hear any thoughts on the whole SPAC model, which really doesn't appear to have taken off, at least not in the health care industry.
Monday, June 25, 2007
Roche makes Ventana an offer it may or may not be able to refuse: $3 billion
As the market in the US closed today, Roche offered to buy the histopathology company Ventana Medical Systems for $75 per share, or about $3 billion to complement its in vitro diagnostics business. The bid is a 44% premium to Ventana's share price last Friday.
 Meanwhile, there's a call for investors tomorrow--more to come.
Meanwhile, there's a call for investors tomorrow--more to come.
Big Week For the Bushes

 While President Bush hosts Russian President Vladimir Putin at the family’s tiny Kennebunkport bungalow , Jonathan Bush, a first cousin of the president, is having a fairly big week himself. Athenahealth Inc., the company he co-founded and leads, filed to go public. One of the few success stories to emerge from the e-health mania of the late 1990s, the Waltham, Mass.-based company—which manages billing and collections for physician offices—hopes to sell up to $86 million in stock. Athenahealth is a service, rather than a software company, although its service is Internet-enabled. Why bring this up in the IN VIVO blog? First, it gives us a chance to run dueling Bush photos. Second, Jonathan Bush matches his cousin in swagger and has suggested in the past that VCs don’t have the fortitude to invest in health care services/IT companies like his. We recently wondered aloud whether David Brailer's new $700m effort will alter that perception. Third, this will be an important IPO. A poor showing could be a setback for the health care IT/services industry.
While President Bush hosts Russian President Vladimir Putin at the family’s tiny Kennebunkport bungalow , Jonathan Bush, a first cousin of the president, is having a fairly big week himself. Athenahealth Inc., the company he co-founded and leads, filed to go public. One of the few success stories to emerge from the e-health mania of the late 1990s, the Waltham, Mass.-based company—which manages billing and collections for physician offices—hopes to sell up to $86 million in stock. Athenahealth is a service, rather than a software company, although its service is Internet-enabled. Why bring this up in the IN VIVO blog? First, it gives us a chance to run dueling Bush photos. Second, Jonathan Bush matches his cousin in swagger and has suggested in the past that VCs don’t have the fortitude to invest in health care services/IT companies like his. We recently wondered aloud whether David Brailer's new $700m effort will alter that perception. Third, this will be an important IPO. A poor showing could be a setback for the health care IT/services industry. Now back to your regularly scheduled pharma discussion.
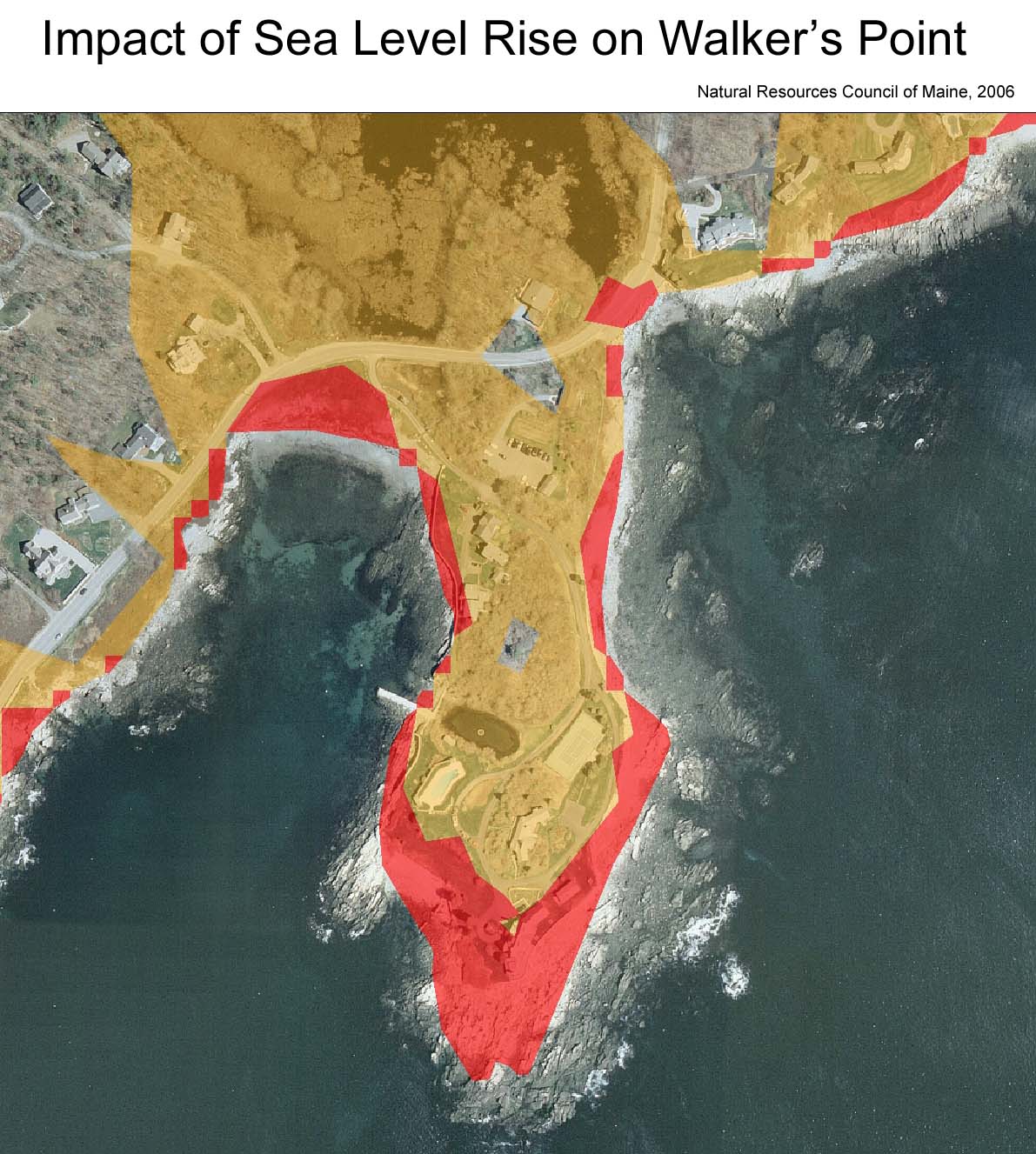
p.s. In case you were wondering what global warming could mean to future Bushes. We suspect the Crawford Ranch is safe.
Venture Debt in Europe: Opportunity Missed?
 European biotechs may bemoan their funding disadvantages relative to US counterparts—the lack of specialist investors, fragmented public markets, poor liquidity and meagre or non-existent PIPEs—but some of the trouble is of their own making.
European biotechs may bemoan their funding disadvantages relative to US counterparts—the lack of specialist investors, fragmented public markets, poor liquidity and meagre or non-existent PIPEs—but some of the trouble is of their own making.
They’re simply not seizing the alternative funding options available to them—such as venture debt, for instance. At least, that was the message from a panel of—you guessed--venture debt providers, speaking at the UK’s BioIndustry Association's BioFinance Europe 2007 meeting last week.
Venture debt has been going strong in the US for at least 20 years; it offers VC-backed companies the opportunity to leverage their equity capital by borrowing quickly, non-dilutively, without affecting valuation, and usually without relinquishing any board seats or voting rights. Last year the US life sciences sector borrowed about $1 billion of this kind of money, according to executives at venture debt providers ETV Capital and GE Financial Services. In Europe, the equivalent figure was less than $50 million.
So what’s going on? That's what the debt providers wanted to find out.
Emotions and ignorance were the top two answers from the panel discussion. The emotional barrier is that these debt providers need to secure their loan—naturally enough—and typically do that against a company’s IP. At a minimum, borrowers may have to sign a “negative pledge” promising not to use their IP to raise debt elsewhere during the course of the loan. But since IP is what the CEO-founders have often spent several decades creating, they’re not, in general, keen to mortgage it, the panellists suggested.
Lack of confidence is another way of putting it: European biotech management and VCs see venture debt as too risky, was the suggestion, because they don’t think they will be able to create sufficient value to pay back the loan—and thus fear that their assets will be seized.
And indeed, venture debt isn’t a lifeline for struggling companies. It’s intended for firms that expect to create value in the near to mid-term and need tiding over—for “high return” situations, as one debt-provider explained in his presentation. If the borrower isn’t in a (relatively) strong position, the deal gets too risky for the lenders. “Companies must have VC support and more than 12 months’ cash” to qualify for venture debt, noted the panellists.
They’ll need enough cash to pay back the loan, too—plus up to 14% interest, and the legal fees associated with the loan. As in any business sector, creditors take priority over the shareholders if things go pear-shaped, which is why management does need to be pretty sure the next round is an up-round, or that the exit they’re after comes at a nice premium. The debt providers require that confidence, too: none will lend without taking share warrants so that they can participate in the hoped-for value creation and meet their return criteria.
Still, for any company not on its knees, venture debt offers “an option to use someone else’s money to create equity value,” the debt providers argued, at least if you think you can create more value than the cost of the loan, and do so before you need to pay it back.
But on to the other reason venture debt hasn't caught on in Europe: management and VCs in Europe just don’t get debt, according to Peter Keen, a partner at VC firm Esprit Capital Partners, chairing the panel. “When you start talking about debt, their eyes glaze over,” he says. Apparently your average European biotech board meeting doesn’t often include a discussion of cost-of-capital, either—and if it does, “that goes right over their heads,” Keen continues.
Here’s the thing: equity is more expensive than debt in many situations. Equity investors expect a 20-30% return (or they used to). Even expensive debt may not cost half that—provided, of course, you can pay it back. So sometimes it’s cheaper, and therefore makes sense, to use debt rather than equity to fund capital expenditure and working capital.
A few European firms have cottoned on. Arrow Therapeutics took a £4 million venture loan to help tide it over while considering its exit options—it was in the end acquired by AstraZeneca for $150 million, so had no trouble with repayments. UK firms Vectura (now public) and Domantis (now part of GlaxoSmithKline) have also used venture debt in the past, according to the panelists, both in order to buy time during financing negotiations.
But these are exceptions. So far, the rest of the UK and European biotech sector either doesn’t like debt, doesn’t get debt, or doesn't feel confident enough in future value creation to take it on.
This may soon change. Public investors, the conference heard, are exiting biotech, not entering. The few specialist funds that exist in the UK and Europe by and large haven't made great returns on that portion of their holdings. US and foreign investors are blocked by pre-emption rights, granting existing shareholders the right to maintain their ownership share in any capital increase. PIPEs are frowned upon (and not easy to do, also because of pre-emption rights).
So soon enough UK and European biotechs may have no choice but to look more pro-actively at alternative financing sources, including venture debt. Especially as M&A continues to offer the prospect of future value-creation.
Meanwhile the inexorable rise of private equity, across all sectors, may help change attitudes too. If anyone knows how to do debt, private equity does. And they’re all getting rich, so eventually perhaps the love-debt message will trickle down to biotech.
Sunday, June 24, 2007
While You Were at ADA
 Here are a few of the stories that IN VIVO Blog picked up on over the weekend ...
Here are a few of the stories that IN VIVO Blog picked up on over the weekend ...
- Not technically a weekend event, but late on Friday Congress introduced legislation that would change the tax treatment of carried interest from a capital gain to regular income, effectively jacking up the tax rate on VCs, hedge funds and private equity shops from 15% to 35%. Spirited discussion continues over at PE Hub, but comments encouraged here too. Will this truly hurt the pace of innovation in the US, as has been and will be argued? Or are undertaxed investors only looking out for #1? Both?
- The American Diabetes Association's annual meeting kicked off in Chicago. Among the companies presenting data was Merck. Reuters reports on some new Januvia data that suggests the drug added to standard therapies (study 1: metformin, study 2: metformin plus sulfonylureas) improves blood sugar better than those therapies alone. The incidence of hypoglycaemia, however, was up in the Januvia groups in each study when compared to the control.
- In other ADA news, Lilly and Amylin presented solid data from a long-term study of Byetta, including progressive weight loss over a three and a half year period. Novo Nordisk's liraglutide is no slouch either. See this June IN VIVO story for the low down on Novo's diabetes prowess.
Friday, June 22, 2007
Brailer's New Quest
 IN VIVO Blog had the opportunity to talk with David Brailer in a previous professional life. He’s thoughtful, intelligent, and proved to be a very good pick to be the federal government’s first health care IT czar. He gave a face to the important need for IT and health care integration, and it’s a concept that has since stuck with the American public.
IN VIVO Blog had the opportunity to talk with David Brailer in a previous professional life. He’s thoughtful, intelligent, and proved to be a very good pick to be the federal government’s first health care IT czar. He gave a face to the important need for IT and health care integration, and it’s a concept that has since stuck with the American public.
In that conversation, which came after he’d already announced his decision to resign his post and go back to California, Brailer more than hinted that private equity or venture capital might be in his future. Smart money had him joining an established firm, probably some big name technology investor with a fair amount of dough already being invested in multiple industries. Brailer, in this scenario, would head up a foray into health care-IT investing, and he’d be a great pick to do so.
What was not envisioned, however, is what actually happened. The California Public Employees' Retirement System--eager to find new technologies to save money on its $4.9 billion in annual health care costs--gave Brailer $700 million from Calpers to invest in health care-IT and health care services companies.
Acccording to reports like this one in Modern Healthcare, Brailer's new firm, Health Evolution Partners, will invest $500 million of that money directly into companies. The rest will go into a $200 million fund of funds that will be committed to other venture firms that invest in the space.
Okay. Does this concern anyone?
No knock against Brailer. He isn't an experienced investor, but he's got street cred, clout and spent the past 15 years doing some level of due diligence. In 1992, he founded CareScience Inc., a supplier of technology tools used in practice management and patient care. He took it public in 2000. But he resigned in 2003 citing differences with the board over the strategic direction of the company. This opened the door for him to be Health Care-IT Czar, giving him an extraordinary perspective on the industry.
But…
Is this sector, which just emerging from the hangover of the "e-health days" of 1999-2000, going to be able to absorb $700 million? According to the published reports, Brailer expects to run through this dough in five years or less. That's $100 million per year or roughly 10% to 15% of what's gone into the health care IT sector and health care services sectors over each of the past two years, according to VentureOne. That’s an enormous influx of cash in a sector that only recently has begun showing some nice returns, albeit mostly on the clinical/hospital sides with companies like Visicu and Emageon.
Perhaps the Internet bubble has us conditioned to think that too much money is always a bad thing. Maybe this is just what the health care-IT czar ordered, a shock of cash to give this somewhat moribund business new life.
But is this good investing? Calpers, according to the reports, is more interested in finding companies with technologies that may someday save it money rather than making money on investments. This sounds an awful lot like a corporate venture capital program in which the parent company is more interested in identifying new technologies than seeing returns. But those corporate investors bring a lot more to the deal than capital. They bring distribution, marketing and usually an established customer base along with decades of expertise.
Brailer brings some of that to the deal, no doubt. He's promising discipline. He told the Sacramento Bee. "We're not going to give them money and say, 'Good luck.' It's going to be very hands-on with these companies." And Calpers could be a huge help if it quickly adopted the products put forth by Health Evolution Partners' portfolio. Brailer, in fact, boldly suggested to the Sacramento Bee that Calpers members could begin benefiting from these advances as soon as next year. (We placed a call at Health Evolution Partners and hadn’t heard back yet. We hope to run an interview with Brailer in an upcoming post.)
The fear here is Calpers is throwing money at a complex problem, and that money will be wasted because the infrastructure—customers, public investors, other sources of capital, regulatory freedom—just isn't in place to support these businesses. It certainly helps that they signed a talent to do the throwing for them. But time will tell whether money is all that was missing.
Thursday, June 21, 2007
The Wrong Man for This Job
 Sometimes the right person comes along at the wrong time. Unfortunately, that appears to be the case with Dr. Andrew von Eschenbach and his stewardship of the Food and Drug Administration.
Sometimes the right person comes along at the wrong time. Unfortunately, that appears to be the case with Dr. Andrew von Eschenbach and his stewardship of the Food and Drug Administration.
Von Eschenbach was persuaded to come over from the prestigious National Cancer Institute to take the helm at FDA during troubled times. He answered the call to duty. His predecessor, Lester Crawford, pled guilty to two misdemeanors for withholding financial information related to food and drug stocks he owned (I wish I was making this up) and the public had lost trust in one of the most important federal agencies in the country. He seemed like the perfect choice to usher the agency through the final years of the Bush Administration.
With the Vioxx controversy seemingly behind the agency, it seemed like FDA had somewhat smooth sailing ahead for the twighlight years of Bush II. Uh, not so much. Results from the Institute of Medicine study on drug safety, the controversies over Sanofi-Aventis' antibiotic Ketek and GlaxoSmithKline's diabetes drug Avandia, and the re-emergence of whistleblower David Graham, among others, contributed to chipping away at FDA's credibility.
Now, more than ever, FDA needs strong leadership. And by strong leadership, I mean an authoritative voice with a clear message. I wrote a piece on this very subject in the June issue of The RPM Report. I'll let you judge for yourself: if you want to read it, click here, and as always, I would love to hear what you out there in the blogosphere have to say.
One of the misconceptions about this issue is that it's an inside-the-beltway issue. Wrong. This is a commercial issue for the pharmaceutical and biotech industries. Don't believe me? Look what the article of one clinical researcher did to GSK's stock. Would the stock have dropped billions in market cap if the docs, the media, the public and the investment community trusted FDA as the final word on drug safety? No doubt, Glaxo's stock price would have taken a hit, but a $13 billion hit in one day?
And that's why, in my opinion, FDA's credibility gap-real or perceived-ranks as the number one business problem for drug manufacturers for the foreseeable future. The credibility gap has infused arguably unprecedented unpredictability into the drug development system, and until it is somehow fixed, that unpredictability will hover over the agency, and only loom larger.
Overheard at the London Stock Exchange Mediscience Awards Dinner
![]() IN VIVO Blog went to tonight's LSE Mediscience awards dinner in London. A quick anecdote:
IN VIVO Blog went to tonight's LSE Mediscience awards dinner in London. A quick anecdote:
Person 1: "They sold their drug to Sanofi-aventis."
Preserving the Right to Advertise—No Matter How Dumb it May Be
 James Madison's Legacy?
James Madison's Legacy?Score another one for the lobbyists at Big Pharma and their allies on Madison Avenue: the House is poised to join the Senate in passing legislation that will put new restrictions on direct-to-consumer advertising—but without putting any moratorium on the right to advertise new products.
The House followed the Senate in bowing to concerns that giving FDA the explicit authority to prohibit DTC ads for new products raises significant Constitutional issues. So, like the Senate, the House bill will now move forward with language allowing FDA to preclear ads, to require disclaimers to prevent false or misleading promotions, and--perhaps most significantly—to levy fines for ads it deems violative.
But the moratorium idea—initially supported by heavyweights like Senator Ted Kennedy and Representative Henry Waxman—is officially dead.
Am I the only one who doesn’t see what the fuss is about?
Don’t get me wrong. We here at the IN VIVO Blog are HUGE fans of the First Amendment.
I just think this ship has already sailed. FDA may not be getting the authority to prohibit DTC for new products, but does anyone in industry seriously expect to be running massive TV campaigns for new drugs again any time soon? Why would they want to?
The Pharmaceutical Research & Manufacturers of America has already conceded the principle behind the moratorium proposals. The association’s voluntary DTC code states that, “in order to foster responsible communication between patients and health care professionals, companies should spend an appropriate amount of time to educate health professionals about a new medicine or a new therapeutic indication before commencing the first DTC advertising campaign.”
The PhRMA code does not specify a minimum waiting period. A one-size-fits-all policy would keep patients from learning important medical information for products that can be safely advertised, PhRMA says. (Oh, and you will be glad to hear the code is working just great. At least PhRMA says it is.)
At first glance, it is easy to understand why Big Pharma would still resist legislative change. After all, a three-year moratorium (as proposed initially in the House bill) enacted by Congress is a lot stricter than the voluntary code adopted by PhRMA.
Except that there really isn’t a difference. The three-year moratorium is the maximum that FDA could require. The minimum would be no waiting period at all for new drugs where FDA saw no issues with immediate DTC.
Plenty of people worry—with good reason—that FDA would err on the side of caution and limit DTC routinely, and presumably put the maximum limit on as often as possible. Sponsors, in effect, would have the burden of proving to FDA that ads would do more good than harm.
The thing is, that sounds to me like exactly the situation industry is in today. FDA may not have the explicit authority to prohibit DTC for new drugs, but they have asked for and received “voluntary” commitments by manufacturers not to advertise as a condition for approval. Sponsors could just to ignore those commitments and FDA would probably be powerless to stop them—but anyone who does that better be ready for the backlash.
And it doesn't take a broken commitment to trigger a backlash.
When an FDA advisory committee recently met to discuss the safety of erythropoiesis stimulating agents in treating cancer patients, there was palpable anger on the committee about Johnson & Johnson’s advertising of Procrit. Committee members felt that J&J's commericials implied a quality of life benefit not found in product labeling. There is no way to prove it, but my hunch is the committee would not have been as tough in its recommendations to restrict ESA labeling if they weren’t so concerned about J&J’s ads.
Then there are the broader implications of the FDA legislation itself. The DTC moratorium may be gone, but the new law will still give FDA a much stronger hand to put restrictions on the roll-out of new products. The era of the billion-dollar blockbuster launch may not be over, but those products are already far rarer than they were, and the new law will make them rarer still.
Far more common will be slow builds, where products spend a year or two on the market in limited use. Only when FDA and the sponsor agree the safety profile allows for it will products break out into broad patient populations.
So why would anyone want to run big TV campaigns for new drugs right after they reach the market anyway?
One way or the other, sponsors need to be prepared to prove that their ads do more good than harm. FDA may not have the authority to demand proof, but the agency—or frustrated members of Congress—can still put advertisers in the hot seat any time they want.
Wednesday, June 20, 2007
Sometimes the Bear Gets You: Coley Pharmaceuticals Edition

Coley Pharmaceuticals shares lost more than half their value today after its partner Pfizer discontinued work on its lead lung cancer compound.
The nail in PF-3512676's coffin was an independent data safety monitoring committee's verdict that a mid-trial analysis suggests the compound plus chemotherapy works no better than chemo alone.
PF-3512676, previously known as Promune (and also as CPG7909), was snatched up by Pfizer in 2005 in a deal worth up to $515 million. The compound was supposed to work by triggering the immune system through stimulating toll-like receptor 9 (TLR-9).
This is the second TLR-modulating drug that has crashed out of the clinic after being dealt to a big pharma for top dollar. Novartis bought rights to Anadys's ANA975 drug, a TLR-7 agonist, for hepatitis C only a few months after the Coley/Pfizer deal. That drug's Phase Ib program remains on clinical hold by the FDA after preclinical tox studies unearthed a potential safety signal last summer. Merck also signed a broad TLR deal with Idera in late 2006; that deal is ongoing.
Coley will hold a conference call later this afternoon.
UPDATE: Coley's call provided little in the way of further information specific to '676. Pfizer is leading the data analysis, according to Coley CEO Bob Bratzler, who described the company as "dumbfounded" and "shocked" at the news.
CSO Art Krieg aimed to confine the bad news to these particular trials and drug combinations, saying "this is a setback for this approach to the treatment of lung cancer in these particular combination regimens ... [but] the mechanisms are validated and we don't think the impact of this will be enormous beyond these approaches." Cancer drug development is challenging, he added, and a lot of successful drugs have failed multiple clinical trials before approval.
Perhaps. But the snafu puts Coley in a tight spot. At last glimpse--end of Q1--the firm had $97 million in cash reserves; yesterday's news sunk Coley's market cap to $91 million. Even considering the firm's estimated burn of about $3 million per month, the market is now placing zero value on its technology platform, its partnered projects with GSK and Sanofi-aventis (and the future of the Pfizer collaboration), as well as its various preclinical activities in RA, lupus and oncology. There is blood in the water.
Why No More Roche-Genentechs?
 Another note from the Oxford Bioscience CEO retreat: why can’t more acquisitions follow the Roche-Genentech model?
Another note from the Oxford Bioscience CEO retreat: why can’t more acquisitions follow the Roche-Genentech model?
The question is being raised with increasing frequency. Understandably so: it’s frustrating to biotech CEOs and scientists to watch their creations disappear into what they see as the bureaucratic abyss of Big Pharma. Sure, these disappearances delight VCs, but they don’t do a lot for the employees who worked as hard as they did because they felt they were building something uniquely valuable.
Sometimes those employees are right. If you think about Genentech-Roche, the deal actually saved both parties. At the time unable to invest in research and delivering sub-par commercial results, Genentech would certainly not exist as an independent company today without the Roche reprieve. Neither would Roche, which gets from Genentech products nearly 50% of its sales and 60% of its operating profit growth. Its ownership position in Genentech shares now accounts for 30% of its own market cap.
Indeed, there is virtually no question that the deal was the single most successful transaction in the modern history of pharmaceuticals. Granted by the deal nearly six years of freedom from stock-market concerns, Genentech created a product-development engine which has delivered virtually unprecedented productivity. And Roche reaped the benefits.
So why have there been no repeat successes? Early on, American Home (now Wyeth) bought a majority of Genetics Institute, and American Cyanamid traded some cash and products for a stake with Immunex. Both were attempted variations of the Roche/Genentech deal; so, in some ways, was Novo's spin-off of Zymogenetics, Novartis' acquisition-cum-alliance with Idenix, and GlaxoSmithKline's alliance-cum-put/call transaction with Theravance.
The jury is still out on the last three; only the Wyeth/GI deal can really be said to have worked at all (that’s the source of Wyeth’s biologics business—key to its growth). But it took Wyeth way too long to capitalize on what it had and when it did, it wasn’t with GI as an independent company. Cyanamid disappeared into Wyeth before it could take advantage of Immunex – and Immunex disappeared into Amgen.
When the subject of acquisitions was raised at the Oxford meeting (full disclosure: the Blog was on the panel), it was pretty clear that there are plenty of biotechs which, rather than getting taken out completely, would welcome the chance to continue semi-independent existence. John Dee, former CEO of Hypnion, sold to Lilly a few months ago, said that he would have preferred it; he apparently even discussed the idea in deal negotiations. But it went nowhere.
There are probably plenty of good reasons Roche-Genentech is tough to duplicate. VCs would certainly rather have a simple exit; so would public shareholders. More importantly, while there probably aren’t many Genentechs around, there certainly aren’t many Roches: controlled by the Hoffmann and Oeri-Hoffmann families, the virtually private Swiss company could make big long-term bets without listening to the carping of investors and analysts (“You’re consolidating those losses for how long? And you don’t even get worldwide rights to its programs?”).
Still, Tuan Ha-Ngoc, the CEO of Aveo, noted two interesting candidates for the Roche role: Astellas and Takeda. Both have global ambitions; both have relatively tolerant shareholder bases. Both apparently want to buy into the biotech industry.
So who knows—maybe the next Roche will be Japanese.
Tuesday, June 19, 2007
Size Matters for Specialist Drugs, Too
 Sales force size, that is. ZymoGenetics’ ex-US commercialization deal with Bayer HealthCare on lead recombinant human thrombin didn’t come as a huge surprise: the west-coast biotech had always said it would seek a partner ex-US.
Sales force size, that is. ZymoGenetics’ ex-US commercialization deal with Bayer HealthCare on lead recombinant human thrombin didn’t come as a huge surprise: the west-coast biotech had always said it would seek a partner ex-US.
But what was interesting about today’s deal was that Bayer also gets to co-promote rThrombin in the US for the first three years post-launch, in exchange for up to 20% sales commission plus bonus payments up to $20 million. Now, this is a specialist drug, sure—it was filed in December 2006 as a safer alternative to bovine thrombin for use in helping control bleeding during surgery, and the entire US market is today worth only $250 million or so.
But ZymoGenetics isn’t the only one going after it (which, incidentally, says much about the growing competition even for niche products). It shouldn’t have too much trouble displacing King Pharmaceuticals’ bovine-derived product Thrombin-JMI, given the recombinant drug’s superior safety and convenience. Bovine thrombin has a black box warning due to immunogenicity, which doesn’t affect rThrombin; the Zymo product can be stored for two years at room temperature, unlike some plasma-derived drugs.
But Johnson & Johnson is also on the loose, thanks to a 2004 deal granting the Big Pharma European and then North American rights to Omrix Biopharmaceuticals’ human blood-plasma derived thrombin, which, like rThrombin, is due for approval later this year.
Zymo argues that surgeons don’t like human plasma derived products either, and that the Omrix drug will also likely carry a warning. But a battle pitting Johnson & Johnson versus Zymo's planned 50-strong US sales force looked too one-sided, whatever the products. That helps explain why Zymo’s share price has remained so muted this year.
It also helps explain why Zymo agreed to the three-year US co-promote--even though it was earlier firm in its intention “to commercialize rThrombin in the US on our own”.
Zymo will still be in charge of US pricing and commercialization, and will book US sales. But Bayer’s added muscle will allow Zymo to quickly penetrate the market, converting a maximum number of hospitals to recombinant thrombin as fast as possible, and also countering any threat from J&J. With the support of Bayer’s 70 US sales reps and 25 scientific liaisons, “we’ll have the largest field force in the hemostasis market,” Zymo's president and CEO Bruce Carter said on the conference call following the deal's annoucement, “as well as what we believe to be a superior product.”
As for Bayer: it has long abandoned global, Big-Pharma style ambition in favor of a more specialist focus. Like other mid-sized pharma, it has tried to position itself as a flexible partner that’s willing to consider ex-US rights only—and let’s face it, that’s increasingly all that’s on offer in today’s sellers’ market, as we've discussed in previous IN VIVO articles.
But the Zymo partnership offers a glimpse of how mid-cap pharma may now be able to leverage the size they do have—relative to many a biotechs, anyway—to secure what are effectively global product deals for products with (relatively) low risk.
And the cost isn’t bad either: Bayer pays Zymo $30 million up front, $40 million on approval, and up to $128 million in milestones, most of which are sales based. Ex-US, it’s in charge, and pays Zymo double-digit royalties.
Monday, June 18, 2007
The Other Surge
 If there is one thing the Democrats can’t stand, it’s a Bush Administration sponsored surge, one that they feel reflects ideology triumphing over common sense. No, I’m not talking about Iraq. I’m talking about the recent spike in enrollment in the Medicare Advantage program, under which senior citizens and the disabled can opt out of the government run Medicare program to join a private sector managed care plan.
If there is one thing the Democrats can’t stand, it’s a Bush Administration sponsored surge, one that they feel reflects ideology triumphing over common sense. No, I’m not talking about Iraq. I’m talking about the recent spike in enrollment in the Medicare Advantage program, under which senior citizens and the disabled can opt out of the government run Medicare program to join a private sector managed care plan.
Okay, I know I know. There is no comparison between the Iraq war and the Medicare Advantage program.
But they do have some things in common. After all, they are both a matter of life and death. That may be more obvious in the case of the Iraq war, where soldiers are putting their lives on the line every day. But it is no less true of the Medicare program, which by its very nature is the health care plan most Americans will rely on to care for them at the end of their lives.
Both are costing the Treasury billions of dollars a year. Everyone knows the Iraq war is expensive. (The Defense legislation pending in Congress would set aside $140 billion to fund operations in Iraq and Afghanistan for fiscal 2008). But did you know that Medicare Advantage plans will collect about $95 billion from the Treasury the same year?
And the long term costs are staggering. CBO says that the Medicare Advantage side of Medicare will consume well over $1 trillion in federal spending over the next 10 years.
But what really sets the Democrats off is the feeling that the money is being wasted. The wisdom of the surge in Iraq is a debate I’m happy to leave to the politicians. But in Medicare Advantage, there is no real debate over one fact: the per capita cost for a Medicare Advantage enrollee is higher—by 10% or more—than the cost of covering the same person in the traditional Medicare program.
That certainly seems to fly in the face of the logic of privatizing Medicare. After all, private plans are supposed to be cheaper and more efficient than big government right?
The two surges have something else in common: however easy it may be to argue that the money is being wasted, it is very difficult politically to do anything about it. No one wants to be accused of failing to support the troops in battle. And no one wants to be accused of penny pinching when it comes to health care for America’s senior citizens. The fact is that Medicare Advantage plans spend a lot of money on better benefits for seniors, so any cuts are likely to be very unpopular with voters.
But the Democrats aren’t giving up. In May, there were no fewer than 9 hearings on ideas to improve the Medicare program. They topics covered ran the gamut, but shared a common theme: all would in some way or the other put the brakes on the growth in the Medicare Advantage program.
Okay, so why should pharmaceutical companies care? In the June issue of The RPM Report, we tease out the implications of the Democratic attack on the Medicare Advantage surge. (You can read the story for free by clicking here.)
If the new leaders in Congress are successful, it means tougher times ahead for pharma companies. Why? Managed care plans will have no choice but to squeeze drug prices even more—or get out of the Medicare business altogether. That, frankly, is what a lot of Democrats probably want. Because that means they get to design the Medicare drug benefit they always wanted—one that you can be sure will include much tougher control of drug pricing.
Should Some of these Butterflies Get Eaten?
 Last week, Oxford Bioscience Partners gathered its portfolio CEOs as well as some interested industry friends to its annual meeting in Cape Cod, this time to talk about “Adapting to Change.”
Last week, Oxford Bioscience Partners gathered its portfolio CEOs as well as some interested industry friends to its annual meeting in Cape Cod, this time to talk about “Adapting to Change.”
And change, the program argued, was necessary to success. The best managers adapt to changing circumstances. Caterpillars become butterflies (that was the picture on the program’s cover).
But unlike the relatively predictable lifecycle of that extraordinary insect, biotechs often go through many transformations, all of them expensive, and very few of them ever yielding the economic equivalent of the butterfly’s winged beauty. (See, for example, an interesting New York Times story on – to mix a metaphor – biotech’s zombies.) Instead, many companies continue to transform themselves into the next thing, somehow attracting hopeful new investors along the way to keep them alive.
To get the discussion started, Oxford had invited a group of executives who had taken their companies (Xoma, Enzo, Oscient, GPC and Alantos) through major business transformations. Most of the companies are impressively old—impressively because only one, the 30-year old Enzo Biochem, supports itself on its own cash flow. And Enzo has been at best a moderate success (a 9% compounded increase in its stock price since 1992 – our systems don’t allow us to go back to 1980, when the company went public at a market valuation of $10 million).
Take the changes sketched by Oscient Pharmaceuticals CEO Steve Rauscher and GPC Biotech CEO Bernd Seizinger.
Both companies dumped their original technology strategies, moving into in-licensing shortly after the genomics balloon deflated. Oscient has gone into primary-care marketing; GPC into oncology drug development, having in-licensed, in satraplatin, what has turned into one of the hottest anti-cancer candidates in biotech (and a relatively old compound, to boot). Seizinger was too politic to point out that in 1998 he had been abruptly fired as the CSO of Oscient, then called Genome Therapeutics. Nor did he point out the fact that Oscient, the company that kicked him out, was now trading at a market cap of just $60 million, despite having two marketed products and $32 million in cash. Meanwhile Seizinger’s GPC had a valuation of about $970 million.
You can argue that Oscient’s transformation into a primary care company was hardly the kind of transformation likely to yield a butterfly. Nonetheless, it follows a traditional storyline: it abandoned technology for products; it dumped its management. Panelist and Alantos CEO Keith Dionne dumped his company’s technology six weeks after he’d joined the company. He kept his German scientists; laid off many of the Americans. Enzo is bringing in new management right now to run its operating businesses (although the parent is still run by its founders). And while it has certainly made money on its inventions, it hasn’t made a lot – it only recently won patent priority in court cases over competing protein array and amplification technologies, both of which it developed in the early 1980s. That’s a long time to wait for a return.
But granted the ability and willingness to transform, the real question is why do it in the first place. That was the pertinent point Mark Carthy, an Oxford partner, asked the panel: given the longevity of some of these companies, the dismal returns from their original strategies, and their subsequent twists and turns, how does the investor make money?
“Timing,” was the general, unhelpful, response.
Meanwhile, Keith Dionne only had to show up to give his answer: he’d sold his company to Amgen for $300 million – rather than sticking around and probably having to change strategy again (it was founded as German Therascope AG in 1999, around a Nobel prizewinner’s combinatorial chemistry platform).
With Xoma trading at well below its 1989 price, let alone its nutty genomic-boom pricing, shouldn’t that company have been assigned to other managers – and more pertinently, other owners? Same for Oscient: the transformation led by Rauscher from discovery into primary care marketing is only one of several huge strategic changes since the company’s founding in 1961 as Collaborative Research. And nowhere has it found traction. But it’s always found investors.
Meanwhile, Xoma has raised more than $700 million of investor capital since it was founded in 1980, and will have soon gone through its fourth CEO. But for Pat Scannon, founder and EVP of Xoma, hope springs eternal: the up-tick in his stock price this year, from $2.16 to $3.40 may, he said, portend great things to come. Just like all the other upticks in his share price over the previous 26 years.
While You Were Celebrating Father's Day ...
 IN VIVO Blog picked up on a few things you may have missed over Father's Day weekend.
IN VIVO Blog picked up on a few things you may have missed over Father's Day weekend.
- The NYT magazine ran a cover story on the fine line between drug prescriber and drug pusher for particularly aggressive pain-management physicians.
- Drugs for pulmonary arterial hypertension (PAH) were front and center at FDA. The agency approved Gilead's ambrisentan (Letairis) and (again) rejected Encysive's sitaxsentan (Thelin). Gilead landed US rights to Letairis via its $2.2 bb acquisition of Myogen last year; the drug could soon start picking up market share from Actelion's bosentan (Tracleer).
- JNJ is blogging. GSK is blogging. But why? (Hat tips: Pharmalot and Pharmagossip)
- Finally, private equity continued its inexorable push into biotech companies yesterday as Lexicon Pharmaceuticals announced it would take on $205 million investment from The Invus Group (which may pour in an additional $345 million over the next four years) and $60 million from Symphony Capital. More on this later ...
Friday, June 15, 2007
What Drug Makers Can Learn from Vaccines
 Drug executives worried about rising safety hurdles, demands for larger trials and politicians’ growing influence on drug regulation could do worse than learn from their counterparts in vaccines.
Drug executives worried about rising safety hurdles, demands for larger trials and politicians’ growing influence on drug regulation could do worse than learn from their counterparts in vaccines.
Massive trial sizes and squeaky-clean safety have been part of the game in vaccines for years—since these are products given to millions of healthy individuals. “We’re used to these challenges,” Didier Hoch, President of Sanofi Pasteur MSD (SPMSD) told IN VIVO Blog this week.
And they’re used to dealing with a few of the other challenges drug firms are now facing, too, including demands for sound health economic and epidemiological data to support reimbursement and the need to engage not just with doctors, but a range of other stakeholders, too, including payors, policy-makers, patients and health workers.
And at €330 per person (for three doses), Gardasil knocks down the old theory that vaccines don't command premium prices. (Though it’s still cheap enough, relative to some cancer drugs, for authorities to reimburse, as they have agreed to do in all of the largest European markets, other than the UK.)
Now sure, vaccines have been hot for some years now: bioterrorism and bird flu were just some of the factors that led to a scramble of Big Pharma (and little biotech) into the field; some returning to what they’d earlier cast aside.
They will get hotter still. Scientists are figuring out how to vaccinate against a wider range of conditions--including ones that haven’t even arrived and may never will, like bird flu. As we reported a few weeks ago, Novartis just committed up to $500m for an anti-smoking vaccine from Cytos. SPMSD and others have more novel vaccines, like Zostavax for shingles and post-herpetic neuralgia, in the pipeline.
Meanwhile, FDA and other regulators are becoming increasingly sceptical of drugs that treat the symptoms of disease, and looking for products which get closer to addressing the cause, or progression, of certain illnesses. Preventing them altogether is even better. And cheaper.
Small wonder, then, that Hoch has, over the last couple of years, had a direct reporting line into Sanofi-Aventis’ outgoing big boss, Jean-Francois Dehecq. Vaccines matter (and perhaps even more now, after one-time-potential blockbuster rimonabant’s big stumble).
SPMSD sets one final example that drug firms might take note of: R&D cooperation. Sanofi Pasteur MSD was created in 1994 as a joint venture between Sanofi-Aventis and Merck. Any vaccine in either company’s pipeline passes to SPMSD after Phase II for further development, approval and marketing in Europe.
The JV was set up because vaccines require large up front investments and significant regulatory expertise, including understanding of, and links to, each European government's policy-makers and approval system.
Given the rising costs and falling productivity of R&D in regular drug firms, pooling costs and risks doesn’t seem a bad idea.
Thursday, June 14, 2007
Rimonabant’s Risky Business
 You know a weight loss drug doesn’t stand a chance when even morbidly obese patients are afraid to take it.
You know a weight loss drug doesn’t stand a chance when even morbidly obese patients are afraid to take it.
During the highly anticipated review of Sanofi-Aventis’ rimonabant by FDA’s Endocrine and Metabolic Drugs Advisory Committee yesterday, Lynn McAfee, the director of medical advocacy at the Council on Size & Weight Discrimination, told committee members that rimonabant was far too dangerous a drug to be allowed on the US market.
“This is a very scary drug,” she told the committee. “I lived through Redux and fen-phen and the calls in the middle of the night from dying people. Nobody wants to live through that again.”
Yikes. That’s a pretty damning statement from a group of people who are so desperate for weight-loss options that they spend nearly a $1 billion a year on dietary supplements—products that never cross the desk of an FDA medical reviewer.
But let’s be serious. As the IN VIVO Blog made clear in an earlier post, when a drug is linked not only to depression and suicidiality, but also a litany of neurological adverse events like seizures and multiple sclerosis, you don’t exactly have a slam-dunk on your hands. And did I mention the 50% chance of losing just 5% of your body weight?
So it should have come as no surprise that the advisory committee voted unanimously against approval. Frankly, the only folks that might have expected a different outcome were from Sanofi-Aventis—a company not exactly known for its sophisticated dealings with FDA. It’s common for a drug sponsor to become so invested in a drug that they can’t see the forest through the trees. But on rimonabant, Sanofi is in a totally different place—like la-la land.
That said, as far as advisory committee management is concerned, Sanofi did a surprisingly good job at trying to convince members that rimonabant deserved their seal of approval. Executives stressed no fewer than a half-dozen times that rimonabant was not for everyone, and totally inappropriate for those that have had or currently have psychiatric problems. And they proposed a pretty decent risk management program, including a controlled launch while they worked out the kinks.
But in the end, there’s only so much you can do with a risky drug. And rimonabant, unfortunately for all those obese patients out there, is a really risky drug.
Is FDA Killing Research?
 It sounds crazy. But it’s what Wyeth’s R&D chief Bob Ruffolo fears if the unprecedented political storm currently engulfing FDA continues to force the agency to raise drug safety hurdles.
It sounds crazy. But it’s what Wyeth’s R&D chief Bob Ruffolo fears if the unprecedented political storm currently engulfing FDA continues to force the agency to raise drug safety hurdles.
“Who is going to bring a new, improved version of Avandia to market,” asks Ruffolo, given the likely trial-size FDA is going to request? How will any company be able to prove that their drug doesn’t have the safety issues associated with Avandia, if these (whether or not they are real) only become apparent from Steve Nissen’s meta-analysis of trials involving 28,000 patients?
No drug is risk-free, and no company-sponsored clinical trial can feasibly replicate real-world drug usage over a number of years. Yet people [politicians, patient groups, Public Citizen, and now FDA] "are demanding absolute positive safety,” Ruffolo tells us.
Now sure, comprehensive safety data within the reasonable bounds of clinical trials is crucially important to getting a drug approved. But if, as Ruffolo contends, regulators—whether or not under pressure from politicians and lobbyists—become obsessed with safety and fail to grant equal attention to benefit, there may be little point in even pursuing drug development within certain classes. Hence, “I’m worried that what saw with Avandia will kill off an entire area of research.” (Add, perhaps, CB1-antagonists to the list, since rimonabant was unanimously rejected by an FDA advisory committee yesterday.)
Avandia, like Lilly/Takeda's Actos (which will also get a black box warning following the NEJM report) is a PPAR gamma agonist. Developers of such single PPARs have already had a rocky road: despite many attempts, they remain the only compounds in their class on the market (there used to be three -- until the FDA forced Warner-Lambert (now Pfizer)’s Rezulin off the market). And Avandia and Actos already in 2002 had their labels updated to reflect safety concerns around congestive heart failure resulting from fluid retention. Meanwhile, every one of the next generation dual alpha-gamma PPAR agonists to get close to the FDA has also failed: remember AstraZeneca’s Galida, discontinued last year because of kidney toxicity; or Merck & Co.’s MK-767; or the compound Merck in-licensed to replace it, Bristol-Myers' Pargluva (whose main antagonist, like Avandia's, was Cleveland Clinic's Steve Nissen).
One might argue, given the list of casualties, that the PPAR class is doomed and it is in fact better that researchers leave it well alone. After all, who wants me-toos? We have a couple of PPARs already out there, the safety-scare will discourage their further usage, and that will force the industry to look elsewhere, for ‘real’ innovation.
But ‘real’ innovation and progress don’t generally happen in giant leaps, they happen in increments. There are plenty of reasons for bringing new versions of Avandia to market, Ruffulo argues, just as there are plenty of good reasons to have a variety of Cox-2 drugs, or a palette of cancer treatments. It’s well known that individuals respond differently to the same drug; in cancer, there’s also the issue of resistance.
Getting back to the PPARs: designing drugs that target different ratios of PPAR alpha, gamma and delta receptors might just improve the side-effect issues that Nissen highlighted, if indeed they are worthy of a black box warning. Despite the failures, companies including GlaxoSmithKline and Sanofi-Aventis are still working on next-generation subsets of PPARs, including dual PPARs and PPAR delta agonists.
So why is Ruffolo so riled up? Wyeth doesn’t have a PPAR agonist (it isn't in diabetes), and, for that matter, doesn’t have a Cox-2 either. In fact, Ruffolo contends, the company has been a little more protected than some from the worst of the safety storm around primary care drugs, in part thanks to its focus on more specialist areas like rheumatoid arthritis (and CNS in primary care, where FDA appears particularly open to new treatment options).
But Wyeth has been hit by its fair share of safety crises—including the Women's Health Initiative study in 2002 which apparently showed an increased risk of breast cancer, among patients taking Wyeth's combined estrogen/progestin hormone replacement therapy Prempro. Positive benefits such as a decrease in hip fractures were overlooked, contends Ruffolo. So are more recent data analyses this year reversing some of the earlier findings on heart attack risk. In today's regulatory reality, meta-analyses count when they’re negative on safety, but not when they’re positive on efficacy. In other words, drug labels can only get worse.
The industry itself is partly to blame for this onslaught, though. Its behavior hasn't exactly been squeakly clean--think enquiries into dubious promotional techniques, accounts of negative trials being swept under the carpet, and the 'dodgeball' that reps were encouraged to play with Vioxx when faced with difficult questions.
Ruffolo acknowledges that the industry makes mistakes. But that won't help the sector out of its plight, nor will blaming eager politicians and watchdogs. For that, drug firms should start rebuilding consumer trust. Perhaps this safety storm will push them into doing so--the silver lining in an otherwise black cloud.

{kind=link}
{kind=link}
{kind=link}